
IACC Strategic Plan
For Autism Spectrum Disorder Research
2013 Update


Introduction
Aspirational Goal: Develop and support infrastructure and surveillance systems that advance the speed, efficacy and dissemination of ASD research.
The original IACC Strategic Plan, launched in 2009, was structured around only six Questions. In 2010, the IACC recognized that grouping the topics of research infrastructure, workforce, and ASD surveillance into a separate chapter would highlight these issues that are critically important to research success and help the Committee track investments and evaluate progress in this area in the same organized, rigorous manner that is used in the rest of the IACC Strategic Plan. Over the past 5 years, a total of $158 million dollars has been invested in building and maintaining the ASD research infrastructure to support needed research and surveillance efforts. Many of the original infrastructure needs identified in 2009 have been accomplished, but continued investment is critical in order to develop, maintain, and build on these valuable new resources.
Progress Toward the Strategic Plan Objectives
The IACC ASD Research Portfolio Analyses reviewed projects funded by both government agencies and private foundations from 2008-2012. From 2009-2012, the total funding devoted to projects pertaining to Question 7 was $158 million. On average for each year from 2010-2012, the funding levels for this Question were doubled from the 2009 level ($16 million) and the number of funded projects was also more than twice as high. Additionally, in years 2009-2012, 27 percent of the total funding went toward core/other research projects that were not aligned with the research gaps covered by the 16 objectives in Question 7.
Of the 16 specific objectives within Question 7, 8 objectives addressing basic and clinical data sharing and dissemination, workforce expansion, and model-systems resources met or exceeded the recommended budget and fulfilled the recommended number of projects. Four objectives, concerning documenting the services available in each state, expanding biobanks, and expanding surveillance infrastructure partially met the recommended budget and had a number of projects underway. Four more objectives did not have any funding or projects. Two of these objectives, focused on a needs assessment for database linkage and a funding mechanism for rapid replication of research results, remain a high priority. The objective concerning development of a web tool for prevalence estimates was fulfilled through several projects that encompassed multiple conditions including autism; the intended goal was achieved, although it was done outside the autism portfolio. The intent of the objective to disseminate best practices in service provision through the publication of "Promising Practices" papers was not completed; this goal may have been superseded by other types of best practice dissemination methods (e.g., web pages, tool kits, presentations at conferences), so the objective in its current form was not viewed by the Committee as a high priority to continue.
Infrastructure
Over the past 5 years there has been a significant rise in data sharing among researchers, increased availability of biological samples, expanded surveillance efforts, substantial investment in building the ASD research workforce and major improvement in dissemination of research results to the community.
Databases have been developed to house and provide researchers with access to valuable research data collected from those affected by autism as well as neurotypical subjects. In addition, in 2011 the NIH Office of Autism Research Coordination (OARC) developed and launched a new database, the IACC Portfolio Analysis Web Tool, that gathers data on federal and non-profit supported ASD research-related projects together into one place, enabling broad public access to detailed information about these projects, as well as searching, sorting and graphics to facilitate further analysis and monitoring of progress over time.
The Interactive Autism Network (IAN), developed by the Kennedy Krieger Institute, is a tool designed to match scientists with research subjects to enhance the pace of research. The IAN network has also greatly facilitated rapid research on issues of symptom severity and intervention. For example, in 2011 when concerns about the impacts of autistic wandering behavior were brought to the IACC's attention through a public presentation at an IACC meeting, members of the IACC and other organizations were able to work with the IAN network within a period of 3 months to launch and complete a study involving over 1,200 children utilizing the IAN database. Results of the study indicated that almost 50 percent of children with ASD had wandered.1 In conjunction with this rapid study, a new International Classification of Diseases (ICD-9) code to track autistic wandering in health records was almost immediately implemented and the American Academy of Pediatrics (AAP) issued new guidelines that included wandering in patient-family anticipatory guidance, alerting parents of children with ASD to the prevalence of wandering so that they could take preventive measures.2
developed by the Kennedy Krieger Institute, is a tool designed to match scientists with research subjects to enhance the pace of research. The IAN network has also greatly facilitated rapid research on issues of symptom severity and intervention. For example, in 2011 when concerns about the impacts of autistic wandering behavior were brought to the IACC's attention through a public presentation at an IACC meeting, members of the IACC and other organizations were able to work with the IAN network within a period of 3 months to launch and complete a study involving over 1,200 children utilizing the IAN database. Results of the study indicated that almost 50 percent of children with ASD had wandered.1 In conjunction with this rapid study, a new International Classification of Diseases (ICD-9) code to track autistic wandering in health records was almost immediately implemented and the American Academy of Pediatrics (AAP) issued new guidelines that included wandering in patient-family anticipatory guidance, alerting parents of children with ASD to the prevalence of wandering so that they could take preventive measures.2
The National Database for Autism Research (NDAR), funded by the NIH, is a rich resource that includes genomic data and imaging studies as well as other types of data for use in ASD research. NDAR has become the standard data repository for the ASD research community. In January 2010, the NIH began including an expectation for data sharing in most of its awards, requiring that human subject data be deposited in a broadly accessible database. In 2012, 81 percent of NIH-funded human subjects grants were contributing data to NDAR. NDAR also supports data sharing from other funders of autism research including the Autism Science Foundation, the Centers for Disease Control and Prevention (CDC), the Department of Defense, and the State of New Jersey. NDAR has also now linked to IAN and the Autism Speaks supported Autism Genetic Resource Exchange (AGRE) and Autism Tissue Program (ATP), enabling researchers to access data in those repositories.
To date, NDAR has facilitated the sharing of data on 70,000 research subjects with much more expected in the next 24 months. Also, the rich "omics" (genomics, proteomics, transcriptomics, metabolomics, etc.) and imaging datasets have been de-identified and protected in the computational cloud, enabling an unprecedented array of resources, techniques and computational software to be used collaboratively by the research community. The results of such efforts along with categorization of data into common concepts like IQ, language and executive function enable users to query and pull down data from across multiple sources and disciplines, maximizing the utility of the data and driving scientific discovery. NDAR data have been cited in publications, and access requests have been substantial. Over 300 researchers at 75 laboratories from 10 countries applied for and were granted access to NDAR in 2013.
Aggregated data in NDAR, among its federated partners and the labs sharing data are available to the general public (see NDAR Query).3 NDAR now supports harmonized receipt of all human subjects research data, including clinical, imaging, genomics, proteomics, electroencephalogram (EEG), eye tracking, and task- based functional magnetic resonance imaging (fMRI) data. Figure 1 provides a summary of the shared research subjects data now available in NDAR. The NIMH Repository and Genomics Resource (NIMH-RGR) is another key resource that has played an important role in supporting research by providing access to biological samples from more than 150,000 well- characterized, high quality patient and control samples from a wide-range of mental disorders, including autism. The number of samples in the NIMH Genomics Repository has increased to more than 27,000, many with extensive phenotype/genotype information. The NIMH repository has also started collecting induced pluripotent stem cell (iPS) lines and fibroblasts. In terms of DNA, this represents a two-fold increase since 2008.
In addition to genomics and cell line samples, brain tissue is another critically important resource needed to further autism research. Unfortunately, brain tissue samples have actually declined in number during the past 5 years due to a freezer malfunction in 2012 that resulted in the loss of more than half of the existing samples from the largest autism brain repository in the United States. The brains lost have not yet been replaced in terms of numbers, and it may take several years to fully recover. In 2013, only nine new ASD brains were added to existing repositories. Despite these challenges and setbacks, there is a concerted effort both publicly and privately to increase the number of brain tissue samples. In 2013, NIH launched a new NIH Neurobiobank initiative. This repository will collect and standardize brain tissue samples for research on ASD as well as other brain disorders. The initiative includes a publication to increase awareness of brain donation, "Why Brain Donation? A Legacy of Hope." (PDF - 946 KB) In addition, a group of private funders including the Autism Science Foundation, Autism Speaks, the Nancy Lurie Marks Family Foundation, and the Simons Foundation, recently launched the AutismBrainNet, a multi-site effort to increase the numbers of ASD-specific brain samples. Their efforts will also include an ASD-specific outreach and education plan to encourage tissue donation.
Launch of NDAR Increases Number of Subjects Whose Data are Shared
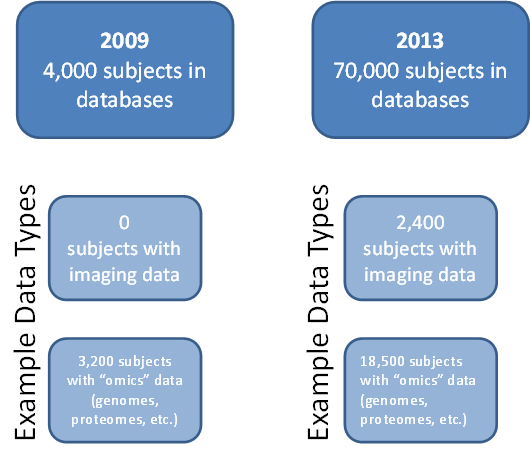
Figure 1. In 2009, essentially all human subjects data being shared within the autism research community were contained in two separate databases—the Autism Speaks AGRE and ATP data repositories—and totaled approximately 4,000 subjects. In 2009, NDAR was collecting data, but its data sharing capabilities were not launched until 2010. Since the launch, NDAR has continued to both collect and make data available to researchers. By 2013, the total number of research participants for whom data were available for study through NDAR had dramatically increased, with data now available for 70,000 subjects. This includes data collected by NDAR as well as the AGRE and ATP datasets, all of which are now available through NDAR. In addition, by 2013 a wide variety of data types was available, with many subjects in the databases having multiple data types available. Examples of the kinds of data shared through NDAR include imaging data, genomes, proteomes, clinical data, and exposures data.
NIMH Repository and Genomics Resource (NIMH-RGR) Sample Summary 2008-2013
| Phenotypic Category |
Number of subjects with DNA/LCL/CPL1 samples |
Number of subjects with samples and phenotypic2 data in distribution3 (% non-caucasian4) |
Number of total affected cases in distribution (independent cases5) |
Number of Multiplex families (Trios) |
Number of subjects with fibroblast lines (iPSC6) in distribution |
|---|---|---|---|---|---|
| Autism (2013) | 28,288 | 15,676 (17%) | 6,278 (4,222) | 1,553 (3,387) | 21 (25) |
| Autism (2012) | 27,240 | 14,628 (17%) | 5,938 (3,906) | 1,530 (3,179) | 0 (0) |
| Autism (2011) | 25,890 | 9,822 (24%) | 4,252 (2,479) | 1,431 (1,860) | 0 (0) |
| Autism (2010) | 23,421 | 8,601 (20%) | 3,842 (2,128) | 1,386 (1,630) | 0 (0) |
| Autism (2009) | 19,824 | 6,434 (19%) | 3,001 (1,598) | 1,125 (1,209) | 0 (0) |
| Autism (2008) | 14,887 | 6,434 (19%) | 3,001 (1,598) | 1,125 (1,209) | 0 (0) |
Table 7. Summary of sample number and type for Autism specific samples included in the NIMH Genomics Repository.1 LCL, Lymphoblastoid Cell Line; CPL, Cryopreserved Lymphoblasts 2 Phenotypic data includes clinical interviews, DIGS (Diagnostics Interview for Genetics Studies) & DSM variables. Samples include unaffected family members.3 Distributions are NIMH sample collections with phenotypic data available for distribution to authorized investigators.4 Non-Caucasians include Black, Hispanic, American Indian and Asian.5 Subjects are unrelated.6 Induced pluripotent stem cell lines produced by NIMH Genomics Repository Stem Cell facility.
Surveillance
Updated estimates published in 2012 from the CDC's Autism and Developmental Disability Monitoring Network (ADDM) indicate that 1 in 88 children has been identified with ASD, based on an average taken across multiple ADDM network study sites across the United States.4 The ADDM network, which uses a methodology based on review of health and education records, has been the CDC's primary United States surveillance initiative. It currently includes 12 sites, and data are now available over multiple years, which enables researchers to examine prevalence trends as well as characteristics that are changing in the population and average age at diagnosis. The ADDM infrastructure has laid the foundation to expand surveillance to younger children in six ADDM sites. In addition, ADDM investigators have initiated data linkage and analytic projects to better understand characteristics of the population of children with identified ASD. These include evaluations of perinatal characteristics, parental age, medication use, participation in the juvenile justice system, hazardous air pollutant exposures, phenotypic characteristics, and changes in prevalence over time, among others. The ADDM Network has established a system to provide updated ASD prevalence estimates and has enabled a better understanding of the needs of the community. In addition to ADDM, the National Survey of Children's Health (NSCH), using telephone survey methodology, reported ASD prevalence estimates that were consistent with ADDM estimates.5 The 2009-2010 National Survey of Children with Special Healthcare Needs infrastructure was used for the 2010 follow-up study, "Survey of Pathways to Diagnosis and Services," to better understand how children with ASD are identified and treated.6 A workshop was held in 2011 to summarize the state of the science and needs in evaluating trends in ASD prevalence.7
There are also many private organizations, and groups outside the United States monitoring prevalence and service data. Autism Speaks has supported a population-based screening effort at an ADDM Network site to evaluate how many children with ASD are potentially being missed by current ascertainment methods. Autism Speaks has also initiated the Global Autism Public Health Initiative (GAPH) to support awareness and epidemiologic studies of ASD in sites around the world. There have also been efforts in the United Kingdom to examine the prevalence of ASD. A study in children using a comprehensive diagnostic assessment method found a prevalence of 1.16 in 100, and a study in adults using a population based survey and diagnostic assessment approach found a similar prevalence of .98 in 100.8–10 In South Korea, a population based study that used diagnostic assessments found a prevalence of 1 in 38, and that two-thirds of cases of ASD identified were unrecognized and untreated, highlighting a need for improved screening, diagnosis and services.11
There is increasing international focus on surveillance of prevalence and services. In 2012, the United Nations (UN) General Assembly unanimously passed a resolution, "Addressing the Socioeconomic Needs of Individuals, Families and Societies Affected by Autism Spectrum Disorders, Developmental Disorders and Associated Disabilities," calling on governments around the world to monitor and report as well as improve access to healthcare, education, training, and intervention programs for persons with ASD and other developmental disabilities.12 In 2013, the executive board of the World Health Assembly, governing body of the World Health Organization (WHO), adopted a complementary resolution, "Comprehensive and Coordinated Efforts for the Management of Autism Spectrum Disorders."13 (PDF - 45 KB) These resolutions indicate growing commitment to address ASD on a global level.
Health disparities are another area of high interest within the field of surveillance. ADDM Network study results initially showed autism prevalence in some minority groups was lower than in in whites, but more recent data have begun to close the gaps with prevalence in minorities and whites becoming more similar, suggesting that the difference is not in actual prevalence but instead may reflect differences in diagnosis (e.g, later diagnosis, missed diagnosis, etc. in minority communities).4,14–16 More research is needed to better understand the role of cultural issues, access to services and other issues in this phenomenon.
ASD is also being studied in immigrant populations to learn more about ASD in diverse populations. In 2013, results from a study of ASD prevalence among diverse populations of children in Minneapolis, Minnesota, collaboratively supported by CDC, NIH, Autism Speaks, and the Association of University Centers on Disabilities (AUCD), showed that while Somali children had a similar prevalence of autism to white children and a higher prevalence than in non-Somali black children or Hispanic children, that the prevalence of intellectual disability among children with ASD was much higher in Somalis.17 Additional studies will be needed to understand the reasons for these differences. A study by Swedish researchers investigated the relationship between parental immigration status and risk of ASD, taking into consideration the importance of region of origin, timing of immigration and autism subtypes.18 They found that children of immigrant parents were at increased risk of ASD with intellectual disability, especially when parents immigrated from countries with a low human development index. That risk was also higher when immigration occurred around pregnancy, but elucidation of the reasons for these differences will require further research.
Despite efforts to track the age of diagnosis and increased capability to diagnose ASD earlier, the average age of diagnosis in the United States has remained relatively constant. The proportion of children being diagnosed earlier has improved, however, with ADDM data indicating that the proportion of children diagnosed by age 3 increased from 12 percent in 2002 to 18 percent in 2008.4 In addition, due to changes in diagnostic criteria and greater community awareness, more cases are being identified when they were initially missed. As the prevalence of ASD has increased, a greater number of children have been identified with ASD — specifically those with ASD without intellectual disability and, as mentioned earlier, among racial and ethnic minority groups. Children without intellectual disability or with fewer ASD characteristics tend to be identified at later ages. Thus, while more children are being identified, much work needs to be done to identify children with ASD and other developmental delays earlier and more equitably so that all of those in need of services can be connected to appropriate services and supports as early as possible.
The surveillance infrastructure may present opportunities for more in-depth data collection related to services, treatment, and co-occurring conditions to complement data currently collected and identify opportunities for improving diagnosis and treatment of children with ASD. A future challenge to the accuracy of trends in prevalence may result from the implementation of the new DSM-5 diagnostic criteria for ASD. Because ADDM has collected detailed descriptions of the clinical findings for each child, the system is poised to evaluate how prevalence estimates may be influenced by these updated criteria.
Future efforts must focus on encouraging more families from diverse backgrounds to participate in ASD research, join registries, and donate biological samples. Also, as the ability to collect and link data grows, it is crucial to pay greater attention to issues of privacy, security and ethical use of data.
Progress Toward the Aspirational Goal
Progress toward the Question 7 aspirational goal to "develop and support infrastructure and surveillance systems that advance the speed, efficacy and dissemination of ASD research" has been rapid over the past 5 years. As demonstrated by the above tables, the numbers of shared subjects and samples have doubled at minimum, and in some cases increased by orders of magnitude. This increase in the availability of resources advances the speed and efficacy of ASD research. The sharing of these resources through initiatives such as NDAR, IAN, and AGRE demonstrate effective dissemination of resources, and fuel the cycle of increased research speed and efficacy. In terms of research infrastructure, the aspirational goal will be met as long as current support is continued and current momentum is maintained.
Surveillance systems have also progressed over the past 5 years, allowing the tracking of prevalence, age of diagnosis, and other trends over time. As awareness of ASD has grown in the community and diagnostic criteria have broadened, more children have been identified with ASD, especially those without intellectual disability and among racial and ethnic minority groups, who tend to be identified at later ages. Thus, while more children are being identified, advances leading to earlier identification for children across all cultural backgrounds and across the entire spectrum and will be critical to ensure that all of those in need of services can receive them as early as possible. With the surveillance infrastructure now in place, there is an opportunity to use it for more in-depth data collection related to services, treatment, and co-occurring conditions to complement data currently collected and identify opportunities for improving diagnosis and treatment of children with ASD.
The progress toward meeting the goal of dissemination and communication of autism research findings has been significant. Many government and private organizations and groups including Simons Foundation, Autism Speaks, Autism Science Foundation, Interactive Autism Network, NIH and the CDC regularly share lay-audience friendly summaries of recent research findings and new interventions to raise community awareness. Future efforts must focus on encouraging more families from diverse backgrounds to participate in ASD research, join registries, and donate biological samples. Throughout the process of ASD surveillance and infrastructure expansion, it will also be important to maintain focus on ethical issues surrounding the privacy of research participants and security of data. The initial steps toward the aspirational goal to "develop and support infrastructure and surveillance systems that advance the speed, efficacy and dissemination of ASD research" have begun, but continued investment and broader outreach will be needed to ensure that the benefits of ASD research and access to the highest quality interventions, services and supports are attainable for all communities across the United States and around the globe.
Question 7 Cumulative Funding Table
| IACC Strategic Plan Objectives | 2008 | 2009 | 2010 | 2011 | 2012 | Total |
|---|---|---|---|---|---|---|
IACC Strategic Plan ObjectivesConduct a needs assessment to determine how to merge or link administrative and/or surveillance databases that allow for tracking the involvement of people living with ASD in health care, education, and social services by 2009. IACC Recommended Budget: $520,000 over 1 year |
20086.4 |
20097.A |
20107.A |
20117.A |
20127.A |
Total$0 |
7.A. Funding: There has been no specific funding for projects addressing this objective. Progress: The Planning Group is not aware of any efforts (projects or funding) that have been made to address this objective since it was created. Remaining Gaps, Needs and Opportunities: A needs assessment remains necessary due to issues surrounding patient privacy in linked databases and also to determine how tracking the involvement of people with ASD in health care, education, and social services is possible with existing tools and resources. It remains to be decided whether this should be a government-led effort or a public/private partnership. Such resources could be utilized by both the research and services provision communities. |
||||||
IACC Strategic Plan ObjectivesConduct an annual "State of the States" assessment of existing State programs and supports for people and families living with ASD by 2011. IACC Recommended Budget: $300,000 each year (revised in 2010) |
20085.1 |
20097.B |
20107.B |
20117.B |
20127.B |
Total$604,013 |
7.B. Funding: The recommended budget was partially met. Progress: Centers for Medicare & Medicaid Services (CMS) conducted a "State of the States" project and released a report summarizing the results of the study in 2014. The book Autism Services Across America Remaining Gaps, Needs, and Opportunities: The initial State of the States study, overseen by CMS, was completed and published in 2014, but the objective calls for an annual study. Since the first study required multiple years to complete and since it is not clear if services will change enough yearly to warrant an annual study, this objective should be revisited with CMS to understand whether an annual study is the best approach. |
||||||
IACC Strategic Plan ObjectivesDevelop and have available to the research community means by which to merge or link databases that allow for tracking the involvement of people in ASD research by 2010. IACC Recommended Budget: $1,300,000 over 2 years |
20086.1 |
20097.C |
20107.C |
20117.C |
20127.C |
Total$13,590,660 |
7.C. Funding: The recommended budget was met. Significantly more than the recommended minimum budget was allocated to projects specific to this objective. Progress: IAN and Group Health Cooperative Autism Registry are two examples of projects that are responsive to this objective. This objective should be considered to be met, with funding exceeding the recommended budget and a large number of diverse projects addressing this issue. NDAR, IAN and AGRE are all publicly available databases. Remaining Gaps, Needs and Opportunities: To advance this objective we need to encourage patients and families to join the registry. Compared to registry numbers for cystic fibrosis (100%), autism is behind at ~4% of patients enrolled in a registry. A table of the numbers of registrants by year would be an informative figure. We need more organized systems to improve participation. |
||||||
IACC Strategic Plan ObjectivesEstablish and maintain an international network of biobanks for the collection of brain tissue, fibroblasts for pluripotent stem cells, and other tissue or biological material, by acquisition sites that use standardized protocols for phenotyping, collection, and regulated distribution of limited samples by 2011.
IACC Recommended Budget: $82,700,000 over 5 years (revised in 2011) |
2008 |
20097.D |
20107.D |
20117.D |
20127.D |
Total$24,752,287 |
7.D. Funding: The recommended budget was partially met. In terms of autism-specific projects, $24.7 million has been spent to date. Including non-autism-specific projects called for in the objective (i.e., the brain atlas), $59.6 million has been spent to date. Progress: NIH launched a new multi-disorder Neurobiobank initiative in 2013. The $5 million effort encompasses autism and other brain disorders, and is not included in the 2008-2012 projects examined by the committee for this update because it began in 2013. A private effort, the Autism BrainNet, is also underway, with several collection/storage/distribution sites governed by a scientific board which distributes samples based on scientific merit of proposed projects to use the tissue. Though these two efforts represent progress, more work is needed to increase the amount of tissues available and to ensure good stewardship of these resources. The BrainSpan Atlas, Remaining Gaps, Needs and Opportunities: While progress has been made in establishing, maintaining and expanding tissue resources for research, this is still an area of enormous need. Currently there may be fewer brain samples available for study than there were at the inception of the Strategic Plan due to the failure of a freezer at a major brain bank in 2012, which resulted in the loss of a large number of ASD brain specimens. There is also still a need for tissue and brains from neurotypical controls. Compared to other disorders, the number of tissue samples available for ASD research is quite low. |
||||||
IACC Strategic Plan ObjectivesBegin development of a web-based toolbox to assist researchers in effectively and responsibly disseminating their findings to the community, including people with ASD, their families, and health practitioners by 2011. IACC Recommended Budget: $400,000 over 2 years |
2008N/A |
20097.E |
20107.E |
20117.E |
20127.E |
Total$1,254,150 |
7.E. Funding: The recommended budget was met. Significantly more than the recommended minimum budget was allocated to projects specific to this objective. Progress: The goal of objective has been achieved in terms of efforts to help researchers more effectively disseminate their findings to the community online and in lay-friendly formats, but not through a web-based toolbox. For example, several agencies, organizations and groups (CDC, NIH, Simons Foundation, Autism Speaks, ASF, IAN) publish lay-friendly summaries of recent scientific findings online, as well as lay-friendly versions of their reports. In addition, the "Data from Papers" feature in NDAR connects readers from the Pubmed citation of a study to the actual data deposited in the database. Remaining Gaps, Needs and Opportunities: Though agencies and organizations are making active efforts to assist researchers with disseminating findings to the community via the web, access to information about research findings remains limited for those communities that are resource-poor and do not have internet access. In addition, the lack of open access to most peer-reviewed journals limits the public's ability to access fully detailed information about new findings. |
||||||
IACC Strategic Plan ObjectivesCreate funding mechanisms that encourage rapid replication studies of novel or critical findings by 2011. No recommended budget assigned by the IACC |
2008N/A |
20097.F |
20107.F |
20117.F |
20127.F |
Total$0 |
7.F. Funding: There has been no specific funding for this objective. Progress: There are no projects categorized to this objective. The Planning Group discussed the issue that creation of funding mechanisms is not likely to be achieved through grant funding, and therefore would not be reflected in the grant portfolio. Remaining Gaps, Needs and Opportunities: The Committee still feels that this objective is relevant and that it is not too early to begin replication studies. In the databases there are 70,000 subjects, 7,000 exomes and 2,500 MRIs that can be used for replication analysis. The intent of the objective was to quickly replicate findings related to potential treatments, but to date, no special fast-track funding mechanisms have been established to support this. |
||||||
IACC Strategic Plan ObjectivesDevelop a web-based tool that provides population estimates of ASD prevalence for States based on the most recent prevalence range and average identified by the ADDM Network by 2012. IACC Recommended Budget: $200,000 over 2 years |
2008N/A |
20097.G |
20107.G |
20107.G |
20127.G |
Total$0 |
7.G. Funding: Autism tracking data is captured in CDC's environmental tracking tool, which became available to the public in 2012, and is not reflected in the autism grant portfolio figure because it is a general tool that encompasses multiple disorders and conditions. Progress: The intent of this objective has been accomplished through the CDC project and can be considered completed. Remaining Gaps, Needs and Opportunities: No new needs or opportunities in this area were identified. |
||||||
IACC Strategic Plan ObjectivesCreate mechanisms to specifically support the contribution of data from 90% of newly initiated projects to the National Database for Autism Research (NDAR), and link NDAR with other existing data resources by 2012. IACC Recommended Budget: $6,800,000 over 2 years |
2008N/A |
20097.H |
20107.H |
20117.H |
20127.H |
Total$9,583,653 |
7.H. Funding: The recommended budget for this objective was met. Progress: The objective to create mechanisms to support the contribution of data from newly initiated projects to NDAR has been met, and NDAR has linked with several other existing data sources such as the ATP, AGRE and IAN. In 2012, 81% of NIH-funded extramural studies were contributing data to NDAR. All NIH grants have terms that require linking of data to NDAR. Remaining Gaps, Needs and Opportunities: Infrastructure will need continued development to enable greater availability of standardized data and analytical tools for cloud computing. IAN data collection could be expanded to include locations of residence to enable geographic data collection on environmental exposures. |
||||||
IACC Strategic Plan ObjectivesSupplement existing ADDM Network sites to use population-based surveillance data to conduct at least five hypothesis-driven analyses evaluating factors that may contribute to changes in ASD prevalence by 2012. IACC Recommended Budget: $660,000 over 2 years |
2008N/A |
20097.I |
20107.I |
20117.I |
20127.I |
Total$23,810,274 |
7.I. Funding: The recommended budget was met. Significantly more than the recommended minimum budget was allocated to projects specific to this objective. (Note that the funding amount for this objective reflects the full funding of the ADDM sites and not just the supplements.) Progress: The research goals in the objective have been achieved. Initially, supplements were needed to support these analyses, but now the ADDM sites are well established and are conducting some analyses using funds from the ADDM grants themselves, while outside supplements are supporting other additional analyses. Remaining Gaps, Needs and Opportunities: Supplements remain an opportunity to capitalize on this infrastructure. |
||||||
IACC Strategic Plan ObjectivesDevelop the personnel and technical infrastructure to assist States, territories, and other countries that request assistance describing and investigating potential changes in the prevalence of ASD and other developmental disabilities by 2013. IACC Recommended Budget: $1,650,000 over 3 years |
2008N/A |
20097.J |
20107.J |
20117.J |
20127.J |
Total$1,369,963 |
7.J. Funding: The recommended budget was met. In addition, the Autism Speaks Global Health Initiative projects address this objective, though they have been coded to their specific scientific areas and are not represented in this funding amount. Also, the CDC provides personnel and help to States, territories and countries as requested, but the budget for that assistance is not reflected in the portfolio analysis figures because this work is not done through grants. Progress: Progress has been made in addressing this need, but not all responsive projects were reflected in the funding amount because some of them were conducted through sources not captured in the portfolio analysis (non-autism specific funding sources) or the projects were assigned according to their scientific topics rather than to this objective. In addition to providing supplemental funding for ADDM site surveillance, Autism Speaks funds projects on surveillance conducted by sites outside of the ADDM network, such as the Kwa-Zulu-Natal Autism Study in South Africa. Remaining Gaps, Needs and Opportunities: While progress has been achieved, ongoing efforts are needed in this area. |
||||||
IACC Strategic Plan ObjectivesEncourage programs and funding mechanisms that expand the research workforce, enhance interdisciplinary research training, and recruit early-career scientists into the ASD field by 2013. IACC Recommended Budget: $5,000,000 over 3 years |
2008N/A |
20097.K |
20107.K |
2017.K |
20127.K |
Total$24,702,276 |
7.K. Funding: The recommended budget was met. Significantly more than the recommended minimum budget was allocated to projects specific to this objective. Many of the fellowship grants are coded according to the specific topic of the research conducted and thus are not represented in this funding figure. Progress: In 2008, NIH supported 46 autism related training/fellowship grants ($5.1 million), and in 2012 NIH supported 78 such grants ($7.7 million). Remaining Gaps, Needs and Opportunities: This objective should continue to be encouraged with a possible future emphasis on services-based research. |
||||||
IACC Strategic Plan ObjectivesExpand the number of ADDM sites in order to conduct ASD surveillance in children and adults; conduct complementary direct screening to inform completeness of ongoing surveillance; and expand efforts to include autism subtypes by 2015. IACC Recommended Budget: $16,200,000 over 5 years |
2008N/A |
20097.L |
20107.L |
20117.L |
20127.L |
Total$3,681,460 |
7.L. Funding: The recommended budget was partially met, but it is noted that the full funding of the ADDM sites is reflected in Objective 7.I. and thus there may be underrepresentation of funding in this category. Progress: Supplements have been provided to six ADDM sites by CDC to collect data from a younger cohort (4-year-olds) in addition to the 8 year olds currently studied; two other ADDM sites have received supplements from CDC to conduct surveillance studies among 15 to 18 year olds. Despite these expansions, further work is needed to better understand prevalence in both younger and older populations. A current project at UNC is reassembling those who participated in TEACCH to conduct a study of long-term outcomes. Also, Paul Shattuck has published studies on young adults with disabilities seeking services that have revealed a significant drop in services use and access post- high school, along with an increased likelihood to remain living with a parent or guardian. In addition, the Utah cohort (mentioned in Question 6) has been used for studies related to adults with autism, with a recent paper identifying health risks and causes of mortality. Remaining Gaps, Needs and Opportunities: While subtypes were included as part of this objective, with the changes in the DSM to eliminate subtypes, this portion of the objective may no longer be relevant. In the future it may be more useful to collect data on characteristics of children and adults with ASD who participate in studies. |
||||||
IACC Strategic Plan ObjectivesSupport 10 "Promising Practices" papers that describe innovative and successful services and supports being implemented in communities that benefit the full spectrum of people with ASD, which can be replicated in other communities, by 2015. IACC Recommended Budget: $75,000 over 5 years |
2008N/A |
20097.M |
20107.M |
20117.M |
20127.M |
Total$0 |
7.M. Funding: There has been no specific funding for this objective. Progress: CMS is no longer supporting the program that produced the earlier promising practices papers; it is possible that other methods of disseminating best practices information are now being used. Remaining Gaps, Needs and Opportunities: Best practices information dissemination is still a high priority, but there may be other means by which this is being done. The focus should be on achieving dissemination rather than on the particular method used. Perhaps this objective should be revisited and replaced with a version that reflects current needs and practices or combined with another objective as appropriate in the future. |
||||||
IACC Strategic Plan ObjectivesEnhance networks of clinical research sites offering clinical care in real-world settings that can collect and coordinate standardized and comprehensive diagnostic, biological (e.g., DNA, plasma, fibroblasts, urine), medical, and treatment history data that would provide a platform for conducting comparative effectiveness research and clinical trials of novel autism treatments by 2012. IACC Recommended Budget: $1,850,000 over 1 year |
2008N/A |
2009N/A |
20107.N |
20117.N |
20127.N |
Total$19,353,505 |
| 7.N. Funding: The recommended budget was met. Significantly more than the recommended minimum budget was allocated to projects specific to this objective.
Progress: Autism Speaks' ATN is a care network that also has research capabilities. The ATN has a collection of biological samples collected from patients who have sought care at the ATN. However, these samples are not targeted toward research use because the samples are not broadly shared like those from other repositories and the samples were not collected systematically. As the ATN has progressed in its work, it has shifted away from the goal of creating a repository to a new focus on developing clinical guidelines, especially in the area of co-occurring conditions. Several guidelines have been published. Another network, the Interactive Autism Network (IAN), has piloted a new rapid method of conducting "virtual" clinical trials of low-risk or "safe" treatments. For example, IAN conducted a trial on omega 3 fatty acids – a commonly used dietary supplement - across 40 states in 10 weeks, demonstrating the value of using interactive research networks for these types of trials. Remaining Gaps, Needs and Opportunities: Clinical and patient social networks represent new ways to conduct research ("practice to research"), as well as a path for evaluating interventions that do not require extensive safety testing (e.g., alternate diets or technological interventions) quickly using large social networks. |
||||||
IACC Strategic Plan ObjectivesCreate an information resource for ASD researchers (e.g., PhenX Project ) to share information to facilitate data sharing and standardization of methods across projects by 2013.
IACC Recommended Budget: $2,000,000 over 2 years |
2008N/A |
2009N/A |
20107.O |
20117.O |
20127.O |
Total$2,404,279 |
7.O. Funding: The recommended budget for this objective was met. Progress: A small number of projects specific to this objective were funded. In addition, there are other projects that are responsive to the goals of this objective, but are coded elsewhere. For example, NDAR has developed a data dictionary that is now widely used across the research community to standardize data terminology so that data can be uniformly shared among researchers. Funding for this project is not reflected in the total for this objective because NDAR is coded elsewhere. NDAR also has a human subject common identifier that is now broadly used by the community. Remaining Gaps, Needs and Opportunities: Funding is necessary to develop standardized methods and protocols. This is a long term project and will need to be approached carefully. |
||||||
IACC Strategic Plan ObjectivesProvide resources to centers or facilities that develop promising vertebrate and invertebrate model systems, and make these models more easily available or expand the utility of current model systems, and support new approaches to develop high-throughput screening technologies to evaluate the validity of model systems by 2013. IACC Recommended Budget: $1,100,000 over 2 years |
2008N/A |
2009N/A |
20107.P |
20117.P |
20127.P |
Total$1,588,780 |
7.P. Funding: The recommended budget for this objective was met. Progress: The project in the Portfolio Analysis that addresses this objective is a NIMH intramural project to produce transgenic mouse models of mental and neurodevelopmental disorders, including ASD. In addition, when mouse models are made under grants and projects coded elsewhere in the portfolio, they are shared via Jackson Laboratories, and that funding is not reflected here. Remaining Gaps, Needs and Opportunities: Emphasis on providing means to encourage development and sharing of animal models, and development of assays that can be used in animal models is still required to advance basic and translational ASD research. |
||||||
IACC Strategic Plan ObjectivesNot specific to any objective (Core/Other Activities) |
2008N/A |
20097.Core/Other Activities |
20107.Core/Other Activities |
20117.Core/Other Activities |
20127.Core/Other Activities |
Total$43,431,065 |
IACC Strategic Plan ObjectivesTotal funding for Question 7† |
2008N/A |
2009$15,809,755 |
2010$50,847,065 |
2011$43,855,291 |
2012$47,516,197 |
Total$170,126,365* |
Table 8: Question 7 Cumulative Funding Table, see appendix for a color-coding key and further details.
* This total reflects all funding for projects aligned to current objectives in the 2011 IACC Strategic Plan and incorporates funding for projects that may have been coded differently in previous versions of the Plan.
† The totals reflect the funding and projects coded to this Question of the Strategic Plan in the particular year indicated at the top of the column. When reading each column vertically, please note that the projects and funding associated with each objective for the years 2008, 2009, and 2010 may not add up to the total at the bottom of the column; this is due to revisions of the Strategic Plan that caused some objectives to be shifted to other Questions under the Plan. The projects and funding associated with these reclassified objectives are now reflected under the Question in which they appear in the 2011 Strategic Plan.
References
1 Anderson C, Law JK, Daniels A, Rice C, Mandell DS, Hagopian L, Law PA. Occurrence and family impact of elopement in children with autism spectrum disorders. Pediatrics. 2012 Nov; 130(5):870–877. [PMID: 23045563]
2 American Academy of Pediatrics. Autism: Caring for children with autism spectrum disorders. (2013). CD-ROM
3 National Database for Autism Research. Query.
4 Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators & Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders--Autism and Developmental Disabilities Monitoring Network, 14 sites, United States, 2008. Morb. Mortal. Wkly. Rep. Surveill. Summ. Wash. DC 2002. 2012 Mar; 61(3):1–19. [PMID: 22456193]
5 Van Naarden Braun K, Pettygrove S, Daniels J, Miller L, Nicholas J, Baio J, Schieve L, Kirby RS, Washington A, Brocksen S, Rahbar H, Rice C; Centers for Disease Control and Prevention. Evaluation of a methodology for a collaborative multiple source surveillance network for autism spectrum disorders--Autism and Developmental Disabilities Monitoring Network, 14 sites, United States, 2002. Morb. Mortal. Wkly. Rep. Surveill. Summ. Wash. DC 2002. 2007 Feb; 56(1):29–40. [PMID: 17287716]
6 Schieve LA, Rice C, Yeargin-Allsopp M, Boyle CA, Kogan MD, Drews C, Devine O. Parent-reported prevalence of autism spectrum disorders in US-born children: an assessment of changes within birth cohorts from the 2003 to the 2007 National Survey of Children's Health. Matern. Child Health J. 2012 Apr; 16 Suppl 1S151–157. [PMID: 22476793]
7 Rice, Catherine E Rosanoff M, Dawson G, Durkin MS, PhD, Croen LA, PhD, Singer A, Yeargin-Allsopp M. Evaluating changes in the prevalence of the autism spectrum disorders (ASDs). (PDF - 838 KB) Public Health Rev. 2012 34(2). [Epub ahead of print]
8 Baird G, Simonoff E, Pickles A, Chandler S, Loucas T, Meldrum D, Charman T. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). Lancet. 2006 Jul; 368(9531):210–215. [PMID: 16844490]
9 Brugha TS, McManus S, Bankart J, Scott F, Purdon S, Smith J, Bebbington P, Jenkins R, Meltzer H. Epidemiology of autism spectrum disorders in adults in the community in England. Arch. Gen. Psychiatry. 2011 May; 68(5):459–465. [PMID: 21536975]
10 Brugha TS McManus S, Smith J, Scott FJ, Meltzer H, Purdon S, Berney T, Tantam D, Robinson J, Radley J, Bankart J. Validating two survey methods for identifying cases of autism spectrum disorder among adults in the community. Psychol. Med. 2012 Mar; 42(3):647–656. [PMID: 21798110]
11 Kim YS, Leventhal BL, Koh YJ, Fombonne E, Laska E, Lim EC, Cheon KA, Kim SJ, Kim YK, Lee H, Song DH, Grinker RR. Prevalence of autism spectrum disorders in a total population sample. Am. J. Psychiatry. 2011 Sep; 168(9):904–912. [PMID: 21558103]
12 United Nations General Assembly. Resolution 67/82: Addressing the socioeconomic needs of individuals, families and societies affected by autism spectrum disorders, developmental disorders and associated disabilities. 2012 Dec;
13 The World Health Organization, Executive Board. Resolution EB133. R1: Comprehensive and coordinated efforts for the management of autism spectrum disorders. 2013 May;
14 Autism and Developmental Disabilities Monitoring Network Surveillance Year 2000 Principal Investigators & Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders--autism and developmental disabilities monitoring network, six sites, United States, 2000. Morb. Mortal. Wkly. Rep. Surveill. Summ. Wash. DC 2002. 2007 Feb; 56(1):1–11. [PMID: 17287714]
15 Autism and Developmental Disabilities Monitoring Network Surveillance Year 2002 Principal Investigators & Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders--autism and developmental disabilities monitoring network, 14 sites, United States, 2002. Morb. Mortal. Wkly. Rep. Surveill. Summ. Wash. DC 2002. 2007 Feb; 56(1):12–28. [PMID: 17287715]
16 Autism and Developmental Disabilities Monitoring Network Surveillance Year 2006 Principal Investigators & Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorders - Autism and Developmental Disabilities Monitoring Network, United States, 2006. Morb. Mortal. Wkly. Rep. Surveill. Summ. Wash. DC 2002. 2009 Dec; 58(10):1–20. [PMID: 20023608]
17 Hewitt A, Gulaid A, Hamre K, Esler A, Punyko J, Reichle J, Reiff M. Minneapolis Somali autism spectrum disorder prevalence project: Community report 2013. (University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living, 2013 Dec).
18 Magnusson C, Rai D, Goodman A, Lundberg M, Idring S, Svensson A, Koupil I, Serlachius E, Dalman C. Migration and autism spectrum disorder: population-based study. Br. J. Psychiatry J. Ment. Sci. 2012 Aug; 201109–115. [PMID: 22361019]